
“There has never been any period in American history where the health of blacks was equal to that of whites. Disparity is built into the system.”
–Evelynn Hammonds, historian of science at Harvard University, quoted in “Why doesn’t the United States have universal health care? The answer has everything to do with race" by Jeneen Interlandi in The New York Times, August 14, 2019
“An antiracist policy is any measure that produces or sustains racial equity between racial groups."
–Ibram X. Kendi, "How To Be an Antiracist," 2019
By Caryl Heaton, DO
“Racism," “racist," and even “anti-racist” are heated words in this culture and in this time. They are hard to hear and hard to apply to ourselves or our state. But a new language is developing that will allow us to listen and learn.
A racist is defined by Ibram X. Kendi, in his 2019 book "How to Be an Antiracist," as “one who is supporting a racist policy through their actions, inactions or expressing a racist idea." A racist policy is “any measure that produces or sustains racial inequity between racial groups." While such definitions of racism can and will be debated, the question of whether our health care system is racist needs to be faced.
How does American health care undermine racial justice?
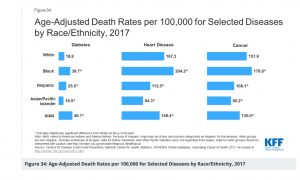
Health outcomes by almost every measure are worse for people of color. For example, Black women have a lower incidence of breast cancer than white women (124.3 vs. 128.1 per 100,000) but the five-year survival of Black women with breast cancer is 80% while the five-year survival for white women is 91%. A Black woman is 22% more likely to die from heart disease than a white woman, 71% more likely to die from cervical cancer, and 243% more likely to die from pregnancy or childbirth-related causes.
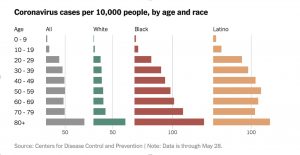
In 2020, Blacks and Hispanics were found to be 2-3 times more likely to die from Covid-19 than whites. (3)
The multiple, complex reasons for this are often referred to as the social determinants of health (SDH). They include economic stability, physical environment, education, nutrition, community/social context, and the health care system. Debating the importance of one determinant above another is a fool’s errand—they are all important. But it is clear that health care coverage, the availability and cultural competency of providers and hospitals, and the quality of care are all critical.
Health insurance that is tied to employment has resulted in higher rates of Black and Hispanic Americans being uninsured. Even the current “safety net” of Medicare and Medicaid have not contributed to equal coverage for all races.
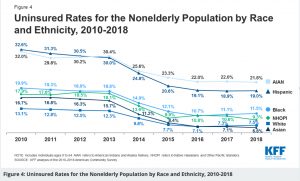
In the U.S. in 2018 the uninsured rate was 7.5% for whites, 11.5% for Blacks, and 19.0% for non-white Hispanics. While these rates have gone down since the passage of the Affordable Care Act, they remain a true disparity. Blacks are 1.5 times more likely to be uninsured than whites and the Hispanic uninsured rate is over 2.5 times higher than for whites.
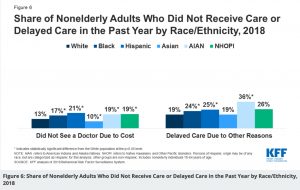
Blacks and Hispanics are more likely to delay or skip care than whites. We don’t have to imagine the reasons—public transportation may be unreliable, child care may be unavailable, low-paying jobs and no time off from work can make the process of getting care difficult.
High deductibles, co-pays, and co-insurance can put care out of reach due to cost. People with lower incomes report poorer health, higher risk of disease, and shorter lives, at every level. (4) A system that produces and sustains these results is a racist system. A system that reduces racial inequality is anti-racist. An anti-racist policy is any measure that produces or sustains racial equity between racial groups.
How would a universal, single-payer health care system be anti-racist?
Health insurance, physician quality, and physician access would no longer be tied to employment or socioeconomic level. Reimbursement for health services would be consistent for all patients and would improve access in underserved communities. In fact, a national health care system could increase access in some rural and urban communities by incentivizing physicians and hospitals to locate there.
Would universal health care improve all social determinants of health? Would it improve nutrition and the bus schedule? Perhaps not, but it works to produce racial equity, and systems where health care is equally provided, such as Medicare or the Veterans Administration (VA), have been shown to greatly improve health outcomes for people of color.
This dynamic can be seen in the case of end-stage kidney disease—an exception to the reality of poor health outcomes for many Black people. Medicare covers that condition regardless of age, and affected Blacks with it survive longer than do whites. In the VA system, Blacks actually have greater longevity than whites. (6) And after the age of 65, when all Americans have health care coverage through Medicare, the disparity in mortality rates between the races starts to lessen. (7)
While the United States struggles with the national crisis of Covid-19, we recognize a second crisis in our country: the struggle of so many who protest and fight against systemic racism and for policies that reduce racial inequities. Central to that struggle is the right to health and a healthy environment. (8)
The establishment of a universal, single-player health care system would provide health care to all, regardless of race, income, disability, prior health conditions, employment status, or immigration status. It would ensure the right to equitable, anti-racist health care in Maine and in America. It would keep us safe and cared for, and it would take us closer to who we, as a people, strive to become.
Caryl Heaton, DO, is a semi-retired family physician and educator who serves on the Maine AllCare Board of Directors. She lives in Downeast Maine.